By Thomas J. Huberty, PhD, NCSP (Indiana University)
Anxiety is one of the most common experiences of children and adults. It is a normal, adaptive reaction, as it creates a level of arousal and alertness to danger. The primary characteristic of anxiety is worry, which is fear that future events will have negative outcomes. Anxious children are much more likely than their peers to see minor events as potentially threatening. For example, giving a brief oral report might be slightly anxiety-producing for most children, but the anxious child is much more likely to believe that his or her performance will be a complete disaster.
Anxious children are likely to engage in a variety of avoidance behaviors to reduce exposure to threat. In the classroom, they may be withdrawn, not initiate interactions, select easy over difficult tasks, and avoid situations where they anticipate increased risk for failure. Socially, they may feel uncomfortable in new situations, not initiate conversations, or avoid group interactions. They worry about being evaluated socially and fear that others will view them negatively. Although there may be some basis for worry, it is usually out of proportion to the situation and is unrealistic. Either a real or imagined threat may be enough to trigger an anxiety reaction.
Defining AnxietyFrom early childhood through adolescence, anxiety can be a normal reaction to stressful situations.
Infancy and Preschool
Anxiety first appears at about 7–8 months of age as stranger anxiety, when an infant becomes distressed in the presence of strangers. At about 12–15 months of age, toddlers show separation anxiety when parents are not nearby. Both of these reactions are typical and indicate that development is progressing as expected. In general, severe stranger and separation anxiety dissipate by the end of the second year of life. Anxiety at this age is primarily associated with fears of strangers, new situations, animals, the dark, loud noises, falling, and injury.
School Age
Up to about age 8, many causes of anxiety continue from preschool levels with a focus on specific, identifiable events. With age, sources of anxiety become more social and abstract, such as worrying about friends, social acceptance, the future, and coping with a move to a new school. Adolescents tend to become more worried about sexual, religious, and moral issues as they continue to develop. In the vast majority of cases, children and adolescents cope well with these situations and severe or chronic anxiety is not common.
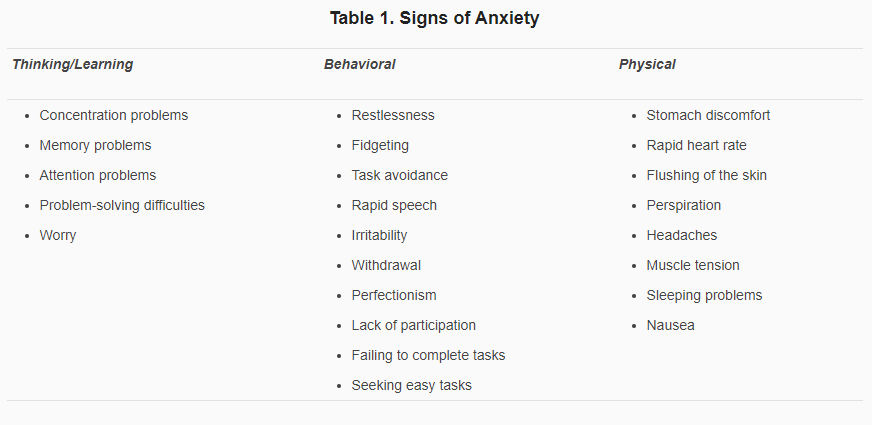
Signs of AnxietyTable 1 summarizes the major thinking/learning, behavioral, and physical signs of anxiety. Not all children will show all signs or show the same signs to the same degree, but a stable pattern that interferes with performance may be cause for concern.
The usual signs of anxiety differ between the anxious and nonanxious child primarily in degree, and may be shown in one or more of the following ways:
Anxiety is one of the most common experiences of children and adults. It is a normal, adaptive reaction, as it creates a level of arousal and alertness to danger. The primary characteristic of anxiety is worry, which is fear that future events will have negative outcomes. Anxious children are much more likely than their peers to see minor events as potentially threatening. For example, giving a brief oral report might be slightly anxiety-producing for most children, but the anxious child is much more likely to believe that his or her performance will be a complete disaster.
Anxious children are likely to engage in a variety of avoidance behaviors to reduce exposure to threat. In the classroom, they may be withdrawn, not initiate interactions, select easy over difficult tasks, and avoid situations where they anticipate increased risk for failure. Socially, they may feel uncomfortable in new situations, not initiate conversations, or avoid group interactions. They worry about being evaluated socially and fear that others will view them negatively. Although there may be some basis for worry, it is usually out of proportion to the situation and is unrealistic. Either a real or imagined threat may be enough to trigger an anxiety reaction.
Defining AnxietyFrom early childhood through adolescence, anxiety can be a normal reaction to stressful situations.
Infancy and Preschool
Anxiety first appears at about 7–8 months of age as stranger anxiety, when an infant becomes distressed in the presence of strangers. At about 12–15 months of age, toddlers show separation anxiety when parents are not nearby. Both of these reactions are typical and indicate that development is progressing as expected. In general, severe stranger and separation anxiety dissipate by the end of the second year of life. Anxiety at this age is primarily associated with fears of strangers, new situations, animals, the dark, loud noises, falling, and injury.
School Age
Up to about age 8, many causes of anxiety continue from preschool levels with a focus on specific, identifiable events. With age, sources of anxiety become more social and abstract, such as worrying about friends, social acceptance, the future, and coping with a move to a new school. Adolescents tend to become more worried about sexual, religious, and moral issues as they continue to develop. In the vast majority of cases, children and adolescents cope well with these situations and severe or chronic anxiety is not common.
Signs of AnxietyTable 1 summarizes the major thinking/learning, behavioral, and physical signs of anxiety. Not all children will show all signs or show the same signs to the same degree, but a stable pattern that interferes with performance may be cause for concern.
The usual signs of anxiety differ between the anxious and nonanxious child primarily in degree, and may be shown in one or more of the following ways:
- Excessive or atypical for age or developmental level
- Inappropriate or excessive for the situation on a frequent basis
- Have persisted for several weeks or months
Anxiety Disorders
A child or adolescent may have an anxiety disorder if anxiety is a pattern causing persistent problems. Several types of anxiety disorders exist, impairing social, personal, or academic functioning. The frequency of anxiety disorders ranges from about 3% up to 20% of children and adolescents. In infancy and preschool children, anxiety disorders are infrequent. They most often start to emerge in early childhood and may persist into adulthood. The frequency of anxiety disorders in boys and girls is about the same during elementary school years, but differences between them emerge in adolescence, with girls being two to three times more likely to develop anxiety disorders. With a 10% frequency rate, a middle school class of 30 students could have as many as three students with an anxiety disorder and perhaps two of them would be girls.
Separation Anxiety Disorder (SAD)
SAD is the only anxiety disorder specific to children and is associated with fears about leaving familiar people, usually parents. In extreme situations, children might refuse to leave their home or not want to stay overnight with a friend. Sometimes, they may refuse to attend school, a pattern often termed "school phobia," although "school refusal" is more accurate. It is not unusual for preschool children to express separation anxiety, but persistent or extreme separation anxiety is atypical for school-aged children and may reflect concerns about family matters, safety, or fears of social rejection.
Generalized Anxiety Disorder (GAD)
GAD is associated with pervasive and high levels of anxiety across a variety of situations with no apparent events that trigger it. It is the most common childhood anxiety disorder and tends to persist to some degree into adulthood. These children often are described as "highstrung" and are often very concerned about doing things well; they may show perfectionist tendencies. The tendency to worry frequently about relatively minor things is a primary defining characteristic of GAD. Children with GAD tend to stay in a relatively high state of physical arousal and often appear stressed much of the time. GAD also tends to be chronic and does not dissipate over time without help, perhaps requiring professional intervention.
Posttraumatic Stress Disorder (PTSD)
PTSD is most often associated with distress as a result of a traumatic situation. The most common types of trauma in children are exposure to violent crime, auto accidents, home fires and injuries, natural disasters, domestic violence, physical and sexual abuse, and serious physical illnesses. Symptoms of PTSD include emotional numbing, avoidance, detachment from others, sleep difficulties, angry outbursts, reliving the experience through stressful memories, flashbacks, and concentration problems. Incidence rates for PTSD symptoms in traumatized children are as high as 20%, and the overall rate in children is about 3%, depending on the circumstances. Girls appear to have higher rates of PTSD than do boys.
Social Phobia
Children who have excessive fear and anxiety about being in social situations and being evaluated by others are experiencing social phobia. The fear of social situations is out of proportion to the actual situation, although some children may not be able to identify specific stressors. The typical age of onset is in adolescence or early adulthood, although shyness and social discomfort can be seen as early as 2 or 3 years of age. Typically, onset is gradual without obvious triggering events.
Causes of Anxiety DisordersConsiderable research has focused on genetic and environmental causes of anxiety. In general, there is a genetic contribution of about 30% in childhood anxiety disorders. It appears, however, that a general tendency toward anxiety is transmitted, rather than a predisposition for specific disorders. Biological influences include temperament, which is a fairly stable personality trait. Anxious children tend to have an inhibited, cautious, and tentative temperament that predisposes them to anxiety disorders. Some anxious children may have differences in certain parts of the brain that affect attention, concentration, and memory. Family factors appear to play an important role, especially from some mothers who overprotect their children, model anxious behavior, and prevent exposure to stressful situations.
Effects on School Performance
Highly anxious children tend to struggle with various demands of school and to be inattentive, perfectionistic, forgetful, or unwilling to participate due to concerns about failure or embarrassment. They may avoid difficult tasks, seek easy tasks, and not volunteer or readily participate in classroom activities. Because withdrawal is a typical response to avoid feeling anxious, anxious children may be perceived by teachers as unmotivated, lazy, or uninterested in school. In fact, the majority of these children want to do well and be involved, but the motivation to avoid feeling anxious is high.
Effects on Social Performance
Anxious children tend to withdraw socially to avoid experiencing anxiety, which leads to further problems of fitting in and making and sustaining friendships. Over time, more social problems and deficits may occur, making the situation worse. Avoidance and worry may offer short-term solutions but have cumulative negative effects and provide little long-term relief.
InterventionsIf severe, anxiety problems may require professional help outside the school. Teachers and parents can ask some initial questions when determining what to do:
School-Based Interventions
Some suggestions for the classroom include:
Home-Based Interventions
Because anxious children also tend to demonstrate these patterns at home, parents can do much to help. Some suggestions include:
Conclusion
Anxiety is a common problem affecting children and adolescents at home and school and can cause significant problems in personal, social, and academic performance. Often, it is not easy to identify, or it may be mistaken for another problem, such as attention deficits, low ability, or lack of motivation. Left unidentified and untreated, it can worsen over time, causing more problems into adolescence and adulthood. Parents and teachers can be major sources of support for anxious children, helping to reduce the negative effects of anxiety and encouraging progress.
Recommended Resources
©2010 National Association of School Psychologists, 4340 East West Highway, Suite 402, Bethesda, MD 20814 (301) 657-0270.
A child or adolescent may have an anxiety disorder if anxiety is a pattern causing persistent problems. Several types of anxiety disorders exist, impairing social, personal, or academic functioning. The frequency of anxiety disorders ranges from about 3% up to 20% of children and adolescents. In infancy and preschool children, anxiety disorders are infrequent. They most often start to emerge in early childhood and may persist into adulthood. The frequency of anxiety disorders in boys and girls is about the same during elementary school years, but differences between them emerge in adolescence, with girls being two to three times more likely to develop anxiety disorders. With a 10% frequency rate, a middle school class of 30 students could have as many as three students with an anxiety disorder and perhaps two of them would be girls.
Separation Anxiety Disorder (SAD)
SAD is the only anxiety disorder specific to children and is associated with fears about leaving familiar people, usually parents. In extreme situations, children might refuse to leave their home or not want to stay overnight with a friend. Sometimes, they may refuse to attend school, a pattern often termed "school phobia," although "school refusal" is more accurate. It is not unusual for preschool children to express separation anxiety, but persistent or extreme separation anxiety is atypical for school-aged children and may reflect concerns about family matters, safety, or fears of social rejection.
Generalized Anxiety Disorder (GAD)
GAD is associated with pervasive and high levels of anxiety across a variety of situations with no apparent events that trigger it. It is the most common childhood anxiety disorder and tends to persist to some degree into adulthood. These children often are described as "highstrung" and are often very concerned about doing things well; they may show perfectionist tendencies. The tendency to worry frequently about relatively minor things is a primary defining characteristic of GAD. Children with GAD tend to stay in a relatively high state of physical arousal and often appear stressed much of the time. GAD also tends to be chronic and does not dissipate over time without help, perhaps requiring professional intervention.
Posttraumatic Stress Disorder (PTSD)
PTSD is most often associated with distress as a result of a traumatic situation. The most common types of trauma in children are exposure to violent crime, auto accidents, home fires and injuries, natural disasters, domestic violence, physical and sexual abuse, and serious physical illnesses. Symptoms of PTSD include emotional numbing, avoidance, detachment from others, sleep difficulties, angry outbursts, reliving the experience through stressful memories, flashbacks, and concentration problems. Incidence rates for PTSD symptoms in traumatized children are as high as 20%, and the overall rate in children is about 3%, depending on the circumstances. Girls appear to have higher rates of PTSD than do boys.
Social Phobia
Children who have excessive fear and anxiety about being in social situations and being evaluated by others are experiencing social phobia. The fear of social situations is out of proportion to the actual situation, although some children may not be able to identify specific stressors. The typical age of onset is in adolescence or early adulthood, although shyness and social discomfort can be seen as early as 2 or 3 years of age. Typically, onset is gradual without obvious triggering events.
Causes of Anxiety DisordersConsiderable research has focused on genetic and environmental causes of anxiety. In general, there is a genetic contribution of about 30% in childhood anxiety disorders. It appears, however, that a general tendency toward anxiety is transmitted, rather than a predisposition for specific disorders. Biological influences include temperament, which is a fairly stable personality trait. Anxious children tend to have an inhibited, cautious, and tentative temperament that predisposes them to anxiety disorders. Some anxious children may have differences in certain parts of the brain that affect attention, concentration, and memory. Family factors appear to play an important role, especially from some mothers who overprotect their children, model anxious behavior, and prevent exposure to stressful situations.
Effects on School Performance
Highly anxious children tend to struggle with various demands of school and to be inattentive, perfectionistic, forgetful, or unwilling to participate due to concerns about failure or embarrassment. They may avoid difficult tasks, seek easy tasks, and not volunteer or readily participate in classroom activities. Because withdrawal is a typical response to avoid feeling anxious, anxious children may be perceived by teachers as unmotivated, lazy, or uninterested in school. In fact, the majority of these children want to do well and be involved, but the motivation to avoid feeling anxious is high.
Effects on Social Performance
Anxious children tend to withdraw socially to avoid experiencing anxiety, which leads to further problems of fitting in and making and sustaining friendships. Over time, more social problems and deficits may occur, making the situation worse. Avoidance and worry may offer short-term solutions but have cumulative negative effects and provide little long-term relief.
InterventionsIf severe, anxiety problems may require professional help outside the school. Teachers and parents can ask some initial questions when determining what to do:
- How typical is the anxiety for the child’s age?
- Does it tend to be situation-specific or pervasive across situations?
- Are there any current events, changes, or circumstances that may help to explain the problem?
- What effects on personal, social, and academic performance are evident?
- What has been tried to help the situation?
- What has helped and what has not helped?
School-Based Interventions
Some suggestions for the classroom include:
- Establish predictable routines
- Set clear and reasonable expectations
- Break tasks into manageable units
- Have specific evaluation criteria
- Provide opportunities for practice and rehearsal
- Pair anxious students with peers who are confident and supportive
- Give special responsibilities
- Give time to relax when anxiety becomes high
- Reduce or avoid unexpected situations
- Avoid punitive and negative attitudes
- Reduce time constraints, if possible
- Move the student to a quiet setting with fewer distractions
Home-Based Interventions
Because anxious children also tend to demonstrate these patterns at home, parents can do much to help. Some suggestions include:
- Be consistent in how you handle problems and administer discipline.
- Be patient and be prepared to listen.
- Avoid being overly critical, disparaging, impatient, or cynical.
- Maintain realistic, attainable goals and expectations for your child.
- Do not communicate that perfection is expected or acceptable.
- Maintain consistent but flexible routines for homework, chores, activities, etc.
- Accept that mistakes are a normal part of growing up and that no one is expected to do everything equally well.
- Praise and reinforce effort, even if success is less than expected. Practice and rehearse upcoming events, such as giving a speech or other performance.
- Teach your child simple strategies to help with anxiety, such as organizing materials and time, developing small scripts of what to do and say to himself or herself when anxiety increases, and learning how to relax under stressful conditions.
- Do not treat feelings, questions, and statements about feeling anxious as silly or unimportant.
- Often, reasoning is not effective in reducing anxiety. Do not criticize your child for not being able to respond to rational approaches.
- Seek outside help if the problem persists and continues to interfere with daily activities.
Conclusion
Anxiety is a common problem affecting children and adolescents at home and school and can cause significant problems in personal, social, and academic performance. Often, it is not easy to identify, or it may be mistaken for another problem, such as attention deficits, low ability, or lack of motivation. Left unidentified and untreated, it can worsen over time, causing more problems into adolescence and adulthood. Parents and teachers can be major sources of support for anxious children, helping to reduce the negative effects of anxiety and encouraging progress.
Recommended Resources
- Anxiety Disorders Association of America: http://www.adaa.org
- Foa, E. B., & Andrews, L. W. (2006). If your adolescent has an anxiety disorder. New York: Oxford University Press.
- Huberty, T. J. (2008). Best practices in school-based interventions for anxiety and depression. In A. Thomas & J. Grimes (Eds.), Best practices in school psychology V (pp. 1473–1486). Bethesda, MD: National Association of School Psychologists.
©2010 National Association of School Psychologists, 4340 East West Highway, Suite 402, Bethesda, MD 20814 (301) 657-0270.
